Hemodynamic response function (HRF) - FAQ
Source: MIT - Mindhive
What is the 'canonical' HRF?
The very simplest design matrix for a given experiment would simply represent the presence of a given condition with 1's and its absence with 0's in a that condition's column. That matrix would model a signal that was instantly present at its peak level at the onset of a condition and instantly offset back to baseline with the offset of a trial. It's possible this may be a good model of neuronal activity, but since fMRI measures BOLD signal rather than neuronal activity directly, it's clearly not that good a model of the hemodynamic response that BOLD signal represents.
If we assume the hemodynamic response system is linear, linear systems theory tells us that if we can figure out the hemodynamic response to an instantaneous impulse stimulus, we can treat our real paradigm as the conglomeration of many instantaneous stimuli of various kind and the hemodynamic response should sum linearly. Tests over the last ten years suggest that the brain does, in fact, largely behave this way, so long as stimuli are spaced more than a couple hundred milliseconds apart. So the canonical HRF is a mathematical model of that impulse response function. It's a function that describes what the BOLD signal would theoretically be in response to an instantaneous impulse. Once your design matrix is described, your analysis software convolves it with a canonical HRF, so that your matrix now represents a gradual rise in activity and gradual offset that lines up with a 'typical' HRF.
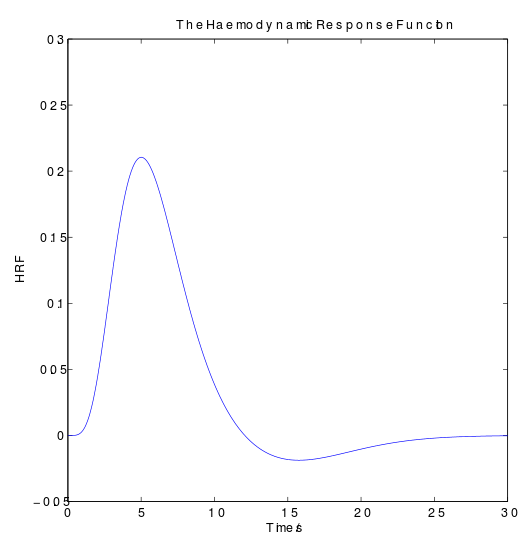
Figure above: Wikipedia
Most of the common neuroimaging programs use similar canonical HRFs - a mixture of gamma functions, originally described by Boynton's group. This function has been found to be a roughly good model of hemodynamic response - at least in visual cortex - in most subjects. It models a gradual rise to peak (about 6 seconds), long return to baseline (another 10 seconds or so) and slight undershoot (around 10-15 seconds), the whole thing lasting around 30 seconds or so.
When should you use the canonical in your model? When should you use different response functions? (HRF, HRF w/ derivatives, etc.) What's the difference?
Generally, the canonical HRF is a decent fit to the true HRF for many normal subjects in many cortical and subcortical regions. If your analysis is intended primarily to test a hypothesis about neural activity, looking only for size and place of activation, and you believe your subjects to be reasonably normal, the canonical makes good sense. If you're looking to find out more about your activation than simply where it is and how big it is, though, you'll need to get a little fancier. Using the canonical HRF will tell you how much the canonical HRF (convolved with your design matrix) needed to be scaled to account for your signal. But you might be interested in more detail - how much variance there was in the onset of the HRF, or how much in its length, or the true shape of the HRF for your subjects. Or you might not think the canonical HRF is a good enough fit to your subjects or your region of interest for you (and there's certainly evidence to make that thought reasonable).
In those cases, you may want to complicate your model a bit. In the extreme, you could not use any sort of a guess at an HRF, and instead directly estimate the shape of your HRF by separately estimating parameters for every timepoint following your stimulus - a finite impulse response (FIR), or deconvolution model. We'll talk about those in more detail later in the course. Alternatively, you might choose to model your neural activity as a linear combination of basis functions like sines and cosines - this will guarantee you can get an excellent fit to your true HRF and use a different HRF at every voxel, thus avoiding the problem of regionally-different HRFs. This is a Fourier basis set model. As an intermediate step between the FIR/basis set - type models and the pure canonical HRF models, you might try modeling your activation as a combination of two or three functions - say, the canonical HRF and its temporal derivative, or dispersion derivative. This will separately estimate the contribution of the canonical HRF and how much variability it has in time of onset (temporal deriv.) or shape (dispersion deriv.).
There are tradeoffs for using the more complicated models: for FIR and Fourier models, the interpretation of any given parameter value becomes very different, and it becomes much more difficult to design contrasts. Using the intermediate steps can get you back physical interpretability, but at the price of decreased degrees of freedom in your data without a guarantee of better fit overall - and, in fact, Della-Maggiore et. al (HrfPapers) find that the HRF w/ temporal derivative has significantly decreased power relative to the canonical alone in a typical experimental design. So use at your own risk...
When does it make sense to do a regionally-specific HRF scan?
If you're particularly interested in a region that's not primary visual cortex and you'd like to get a very good fit of your model to the data, it may make sense to try and get an HRF that's specific to a different region. The canonical HRF is derived from measurements in V1 of some subjects, and studies like Miezin et. al (HrfPapers) have demonstrated that between-region variability within a subject in one scan can be significant.
However, if you're worried about this, rather than taking an entirely separate scan or task to estimate impulse response in a region, it probably makes more sense to use an analysis type that models the response of each voxel separately - like an FIR or Fourier basis set model - which doesn't assume that you have the same HRF at every voxel.
When does it make sense to do a subject-specific HRF scan?
If you're looking to study intersubject variability, or if you're looking to improve the fit of your model by a good chunk and you can afford the extra time in the scanner. Several studies, like Aguirre et. al and Miezin et. al (HrfPapers), have demonstrated there is a significant amount of variability between subjects in several parameters of the HRF - time to onset, time to peak, amplitude, etc.
Perhaps more importantly, the canonical HRF is based on measurements from normal, adult cortex. It's becoming clear that populations like children, the elderly, or patients of various kinds may have HRFs that differ significantly from the canonical. Particularly in any sort of between-group study in which these populations are being compared to normal subjects, it's crucial to ensure that any effect you see isn't driven by the difference in fit of the HRF between groups - you would expect the canonical HRF to provide a better fit (and hence more and larger activations) to normal adults than it would to patients or non-standard populations. In cases like these, using a subject-specific HRF may be necessary or at least desirable.
Which regions have particularly different HRFs?
Probably a lot of 'em. But in particular there are questions about the extent to which the canonical HRF or others measured from cortical neurons maps onto HRFs for subcortical structures like the basal ganglia. Definitive answers about this sort of thing await further study. Logothetis & Wandell (2004; HrfPapers) discuss some reasons why regions might differ in HRF - from increased white matter density to differences in vascular density to, um, complicated physiological things. But they have one clear point: we know HRF can vary from region to region, and there is no accurate way currently to convert the absolute BOLD magnitude to any neural measure. Which means comparing absolute BOLD effect between regions, even nearby, is simply not justified theoretically. In their words:
"It seems that with our current knowledge there is no secure way to determine a quantitative relationship between a hemodynamic response amplitude and its underlying neural activity in terms of either number of spikes per unit time per BOLD increase or amount of perisynaptic activity." - Logothetis & Wandell (2004)
So be cautious about comparing absolute magnitude between regions...
Which populations have particularly different HRFs?
Surprising few studies have been published on this subject. Ongoing studies at Stanford (Moriah Thomason & Gary Glover) suggest children of at least a certain age have important differences in their HRF, and it's clear the same is true of elderly subjects. But at present, if you're interested in using any non-standard population of subjects, it's not a crazy idea to assume they have significant differences in their HRF from the standard canonical.
What's the difference between an 'epoch' HRF and an 'event' HRF?
If you're using AFNI/BrainVoyager/SPM2, there isn't any. So don't worry about it. But if you're using SPM99 or earlier, the story above about the canonical HRF is actually oversimplified. In SPM99 (and earlier), epoch-related and event-related studies had the same underlying design matrix form - the onset of a trial was marked with a 1, but the actual trial itself was all 0's. Event-related studies were simply modeled by convolving those with a canonical HRF, but epoch-related studies clearly needed to account for the length of the trial. So there was a separate, epoch-related, canonical HRF, that was also based off a mixture of gamma functions, but was specifically scaled to account for the length of the trial - so the HRF that was convolved with the design matrix was different for a 12-second epoch and a 30-second epoch. The epoch HRF generally looked like a wider, fatter canonical HRF, and represented a model of linearly summed HRFs over the course of the trial.
With a re-vamping in data structures, though, in SPM2, and further study, this difference was scrapped. Epochs are now modeled differently at the level of the origingal, pre-convolved design matrix, with 1's down the whole length of the trial, and events and epochs are convolved with the same canonical HRF. This seems provide an equally good or better fit to real data as well as simplifying many calculation aspects.
What relationship does the BOLD have to the underlying neuronal activity?
(This should probably be higher up the question list.) The BOLD signal is produced by an influx of oxygenated blood to a local area of neuronal activity, to compensate for increased energy usage. But neurons use energy for a lot of things, both pre- and post-synaptic: action potentials, increased membrane potentials, cleaning up neurotransmitter, putting out neurotransmitter, etc. In order to correctly interpret the BOLD in a given region, we need to know if it's caused by, say, increased firing (i.e., output) or increased post-synaptic activity (i.e., increased input) or some combination. What aspect of the underlying electrophysiology does the BOLD correlate with?
Logothetis & Wandell (HrfPapers) review a good deal of this work. Several electrophysiology studies have found tight correlations between BOLD and local field potential (LFP), a lower-frequency electrical measure summed over many neurons (but still with good spatial resolution). Similarly, fast ERP amplitude seems to vary linearly with BOLD (Arthurs & Boniface (2003), RoisPapers). Slow ERPS, which are believed to arise from _post_synaptic potentials, correlate with BOLD in parietal cortex (Schicke et al. (2006), HrfPapers). Some studies have also found linear relationships between spike rates and BOLD, and spiking activity likely also correlates with BOLD, although perhaps not as robustly (Logothetis et al., 2001).
All this goes to suggest that BOLD may originate less in actual neuronal spiking and more in low-frequency potentials or increased excitability of neurons: in other words, BOLD reflects input to an area more than output. Clearly, input and output are often correlated for neurons; excitatory input will increase spiking outputs. But they aren't always; if this hypothesized connection is true, it means an increased BOLD could reflect increased inhibitory input to a region, or summing of both inhibitory and excitatory inputs (resulting in no change in spiking). Logothetis & Wandell also cite examples where BOLD might be different from single-unit recording - e.g., an area may appear highly direction-sensitive with BOLD, even if single-unit recordings show it not to be, because it is highly interconnected with a very direction-sensitive area. Attention effects, which are difficult to find in V1 with single-unit recordings but show up in fMRI, might be another example. So we should have caution in using models that require BOLD signal to directly index increased spiking outputs.
This is not to say it's impossible to map single-unit firing onto BOLD signal; retinotopy in visual cortex, for example, happens at the single-unit level, and is easily detectable with BOLD. But merely note: many factors, from input activity to vascular density (see above), etc., can affect regional BOLD response.
How does the hemodynamic response change with stimulus length?
In very nonlinear ways. See Glover (1999) in PercentSignalChangePapers (and Logothetis & Wandell, 2004, HrfPapers). You're on very shaky ground if you attempt to model stimuli longer than 6 sec by convolving a standard HRF with a boxcar. You may be better off using stimuli separated by longer times or shorter stimuli.
Hemodynamic response function (HRF) - FAQ的更多相关文章
- 对于fmri的hrf血液动力学响应函数的一个很直观的解释-by 西南大学xulei教授
%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%% clear all;clc; %%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%% ...
- laravel route路由,视图和response和filter
Laravel充分利用PHP 5.3的特性,使路由变得简单并富于表达性.这使得从构建API到完整的web应用都变得尽可能容易.路由的实现代码在 application/routes.php 文件. 和 ...
- Laravel框架学习(Response)
1.Response篇 1.1 基本响应 最基本的HTTP响应只需在路由闭包或控制器动作中返回一个简单字符串即可,但是具体业务逻辑中大部分响应都是在控制器动作中返回Response实例或者视图.Res ...
- Notes: Principles of fMRI 1 (Coursera)
course link: https://class.coursera.org/fmri1-001 Part 1 ❤ Three fundmental goals in fMRI: localiza ...
- fmri 实验设计 / 范式设计/ paradigm design
reference:http://www.psychology.gatech.edu/cabi/Resources/Course/index.html sluggish 懒散的,无精打采的.哈哈,pp ...
- Angular企业级开发(4)-ngResource和REST介绍
一.RESTful介绍 RESTful维基百科 REST(表征性状态传输,Representational State Transfer)是Roy Fielding博士在2000年他的博士论文中提出来 ...
- Promise的前世今生和妙用技巧
浏览器事件模型和回调机制 JavaScript作为单线程运行于浏览器之中,这是每本JavaScript教科书中都会被提到的.同时出于对UI线程操作的安全性考虑,JavaScript和UI线程也处于同一 ...
- webpack搭建前端一条龙服务
作为从grunt.gulp一路走来的老码农,一开始用webpack的时候我是很抗拒的.但由于核心库使用了vue,而webpack又是vue的最佳拍档(vue作者专门为其写了vue-loader),所以 ...
- 后HTML5时代
十二年前,无论多么复杂的布局,在我们神奇的table面前,都不是问题:十年前,阿捷的一本<网站重构>,为我们开启了新的篇章:八年前,我们研究yahoo.com,惊叹它在IE5下都表现得如此 ...
随机推荐
- 匹夫细说C#:可以为null的值类型,详解可空值类型
首先祝大家中秋佳节快乐~ 0x00 前言 众所周知的一点是C#语言是一种强调类型的语言,而C#作为Unity3D中的游戏脚本主流语言,在我们的开发工作中能够驾驭好它的这个特点便十分重要.事实上,怎么强 ...
- php内核分析(七)-扩展
这里阅读的php版本为PHP-7.1.0 RC3,阅读代码的平台为linux. 我们研究下反射这个扩展. 反射这个扩展目录是存在在:ext/reflection.其实里面的代码很简单.一个.h文件,一 ...
- 数百个 HTML5 例子学习 HT 图形组件 – WebGL 3D 篇
<数百个 HTML5 例子学习 HT 图形组件 – 拓扑图篇>一文让读者了解了 HT的 2D 拓扑图组件使用,本文将对 HT 的 3D 功能做个综合性的介绍,以便初学者可快速上手使用 HT ...
- HTML5 网络拓扑图性能优化
HTML5 中的 Canvas 对文本的渲染(fillText,strokeText)性能都不太好,比如设置字体(font).文本旋转(rotation),如果绘制较多的文本时,一些交互操作会手动很大 ...
- C# 条件编译
本文导读: C#的预处理器指令从来不会转化为可执行代码的命令,但是会影响编译过程的各个方面,常用的预处理器指令有#define.#undef.#if,#elif,#else和#endif等等,下面介绍 ...
- Navisworks 2014 Api 简单的使用
初次接触Navisworks Api .NET 的二次开发.主要是研究了一下.关于NavisWorks 结构树的加载. void LoadModel() { //清空当前的结构树信息 treeVie ...
- 运用css,对于下拉菜单的制作
<html xmlns="http://www.w3.org/1999/xhtml" lang="en"> <head> <met ...
- Java 单例模式详解
概念: java中单例模式是一种常见的设计模式,单例模式分三种:懒汉式单例.饿汉式单例.登记式单例三种. 单例模式有一下特点: 1.单例类只能有一个实例. 2.单例类必须自己自己创建自己的唯一实例. ...
- JAVA基础培训(isoft)
我们
- quartz CronExpression表达式
一个cron表达式有至少6个(也可能7个)有空格分隔的时间元素.按顺序依次为1.秒(0~59)2.分钟(0~59)3.小时(0~23)4.天(月)(0~31,但是你需要考虑你月的天数)5.月(0~11 ...